
- The Coverage Lifecycle
- The Pattern Across the Lifecycle
- Why This Has Been Misdiagnosed
- Final Thoughts
Healthcare organizations don't lose revenue because claims are processed incorrectly. They lose it because coverage decisions are made on incomplete information long before a claim exists.
By the time a claim is submitted, most of the outcome has already been determined — whether authorization requirements were met, whether documentation aligns with payer rules, and whether eligibility details were interpreted correctly. What appears downstream as a denial or delay is usually the result of decisions made earlier in the process, without full visibility into coverage requirements.
To understand why this happens, it helps to look at the full coverage lifecycle.
The Coverage Lifecycle
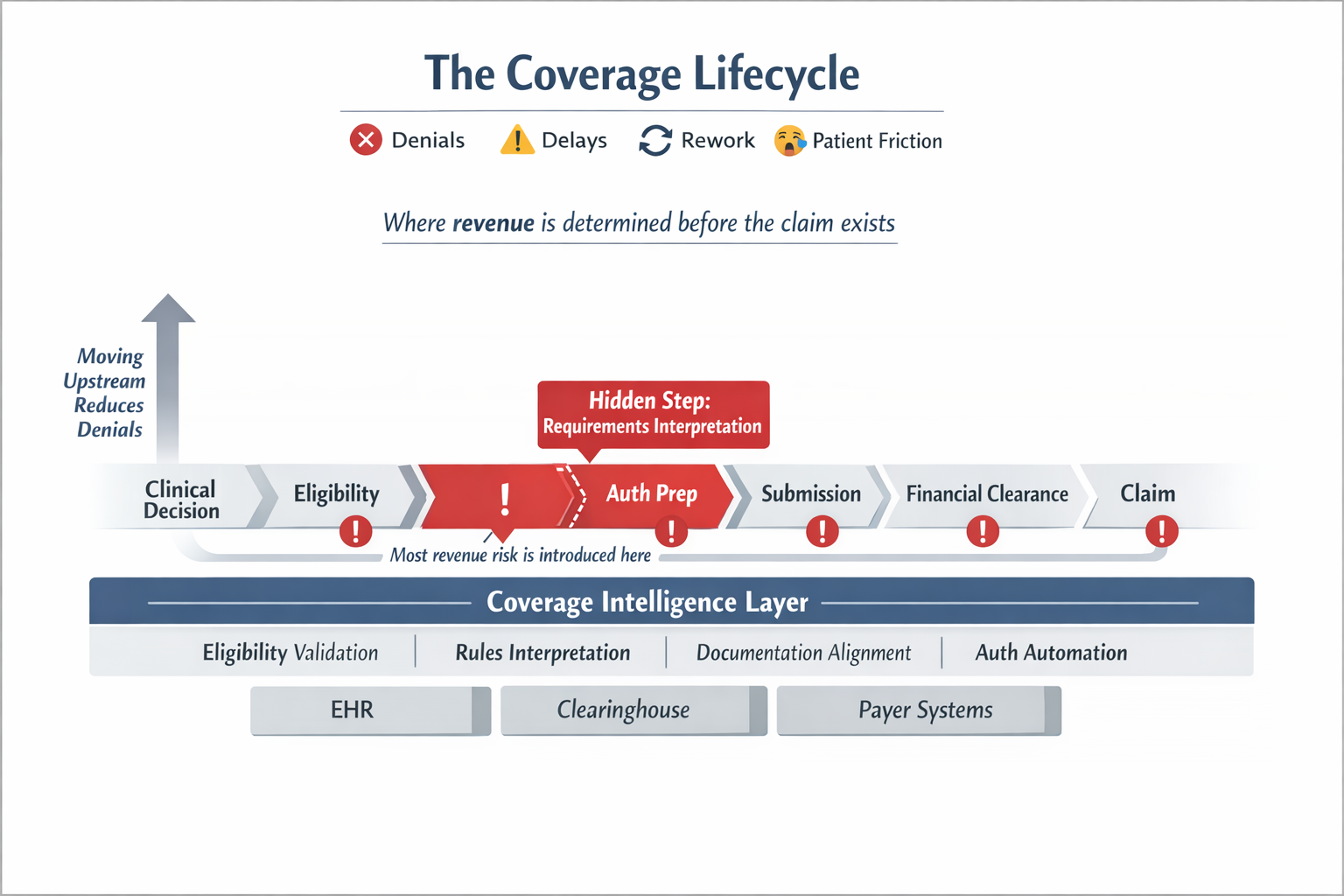
Across specialty and procedural practices, pre-service revenue follows a consistent pattern. Not as a clean workflow, but as a chain of interdependent decisions — each one relying on coverage data that is often fragmented, outdated, or unclear.
Clinical Decision and Scheduling
A provider determines that a procedure or visit is needed. The patient is scheduled. At this moment, a financial decision is being made without full visibility into authorization requirements, payer-specific rules, or patient financial responsibility. Coverage is assumed to be something that can be sorted out later. It rarely is that simple.
Eligibility Verification
Staff confirm insurance coverage through the EHR, clearinghouses, or payer portals. This step confirms coverage status and basic plan information. What it does not provide is procedure-specific requirements, documentation expectations, or plan-level nuances. Eligibility is "verified" — but coverage is not truly understood.
The Step That Rarely Appears on System Diagrams
After eligibility is confirmed, someone has to answer three questions:
- Does this procedure require prior authorization?
- What clinical documentation is needed?
- Which rules apply for this specific payer and plan?
These questions sound straightforward. In practice, they are not. Authorization requirements vary across payers and plans. Rules change frequently — sometimes without notice. The information needed to answer them exists across portals, PDFs, and institutional knowledge that lives in the heads of experienced staff.
The result is that two coordinators reviewing the same case may reach two different conclusions. Neither is acting carelessly. The system simply does not give them a reliable way to arrive at the same answer.
This is not a workflow problem. It is a data and intelligence problem. And because every subsequent step in the lifecycle depends on getting this step right, errors here compound across everything that follows.
Authorization Preparation
Clinical documentation is assembled and structured for submission. When requirements were never fully defined in the previous step, documentation is assembled against incomplete criteria — missing required elements, misaligned with payer expectations, lacking the clinical context reviewers need. Authorization-related issues are a leading contributor to downstream denials, and most of them trace back to this moment.
Authorization Submission and Tracking
Requests are submitted through payer-specific systems. Incorrect submission pathways, limited status visibility, and manual follow-up requirements compound delays. Work expands as staff chase authorizations that should have been clean on first submission.
Financial Clearance
Patient responsibility is estimated and communicated. When coverage requirements were not fully understood earlier in the lifecycle, those gaps surface here — often in the form of unexpected costs that create patient friction and downstream collection risk.
Day-of-Service Validation
Final checks occur before care is delivered. Authorization gaps, coverage mismatches, and missing documentation discovered at this stage result in delays, rescheduling, and lost utilization. These are not close calls. They are the visible end of a chain of upstream misses.
Claim Submission
At this point, the system is no longer making decisions. It is reporting outcomes. Denials tied to authorization issues, documentation gaps, or coverage misinterpretation are not billing failures. They are the visible end of upstream intelligence failures — made legible only after the damage is done.
The Pattern Across the Lifecycle
When you step back, a consistent structure emerges. Each step depends on coverage data. That data is incomplete, fragmented, or changing. Humans are responsible for interpreting it. And errors compound as the process progresses.
This is why organizations experience persistent denial rates, high administrative burden, and unpredictable cash flow — not because their workflows are poorly designed, but because the system lacks a reliable way to understand coverage requirements in real time.
Why This Has Been Misdiagnosed
Most solutions have focused on workflow optimization, labor scaling, and process standardization. These approaches improve throughput. They do not improve decision quality. Even AI-adjacent tools have tended to treat this as an infrastructure problem — a matter of better EHR integration or clearinghouse connectivity — reinforcing the idea that the bottleneck is system integration.
It isn't. The bottleneck is a missing layer of technology that no existing platform was designed to own. We explore this in detail in The Missing Layer in Your Revenue Cycle Technology Stack.
A Different Framing
The coverage lifecycle is not a workflow problem. It is a data and intelligence problem. Specifically: unstructured payer requirements, constantly changing rules, fragmented sources of truth, and no system responsible for interpretation.
Until those conditions are addressed, the same failure patterns will persist — regardless of how efficient the workflow becomes.
Final Thoughts
Healthcare revenue is typically analyzed at the point of denial. But that is the wrong place to look.
The real question is: what did the system know — and not know — when decisions were made earlier in the lifecycle?
Because that is where revenue is actually won or lost.









-cropped.svg)
.svg)