
- The technology stack that runs most specialty practices
- Why the existing stack cannot solve the problem
- Mind the gap
- Why this gap has persisted
- A more complete model of the revenue cycle stack
- What changes when the gap is filled
- The diagnostic test for your own stack
- Final Thoughts
Executive Summary
Most specialty practices run their revenue cycle on three technology layers: clinical systems, connectivity infrastructure, and billing platforms. These tools are well-established, well-integrated, but still insufficient. Between clinical care and claim submission sits an operational layer — coverage verification, authorization management, payer rule interpretation — that no existing platform was designed to own. That gap is not a workflow inefficiency. It is a missing category of technology. And it is where most pre-service revenue is won or lost.
The technology stack that runs most specialty practices
Ask a revenue cycle director to describe their technology environment and you'll hear a consistent answer regardless of specialty, size, or geography.
An EHR for clinical documentation and scheduling. A clearinghouse for payer connectivity and claim transmission. A billing platform for claims management, payment posting, and collections.
This is the standard model. It is also nearly universal — which means when something goes wrong in the revenue cycle, these are the systems that get examined first. New integrations get built. Workflows get optimized. More staff get added to manage the gaps.
But the denial rates stay roughly the same.
Why the existing stack cannot solve the problem
The three platforms that form the foundation of most revenue cycle operations were each designed to solve a specific and well-defined problem.
EHRs store and surface clinical information. They are documentation systems. Their job is to capture what happened clinically and make it available to the people and systems that need it.
Clearinghouses transmit. They are connectivity infrastructure. Their job is to move claims between providers and payers as efficiently as possible, with the format and routing logic that each payer requires.
Billing platforms process and reconcile. They are financial operations systems. Their job is to manage the downstream revenue cycle — claim status, payment posting, denial management, collections.
None of these systems were designed to interpret. None of them were built to answer the question that sits at the center of pre-service revenue: for this specific patient, this specific procedure, and this specific payer — what is required to get paid, and does this practice currently have it?
That question is not a documentation question. It is not a transmission question. It is not a billing question. It is a coverage intelligence question. And there has never been a purpose-built layer of technology responsible for answering it.
Mind the gap
Between clinical care and claim submission, specialty practices perform a set of tasks that are among the most consequential in the revenue cycle — and the least supported by technology.
Determining whether a procedure requires prior authorization for a specific payer and plan. Identifying what clinical documentation that payer's reviewers will need to approve it. Validating that the documentation assembled meets those criteria before submission. Estimating patient financial responsibility with enough accuracy to clear the patient before care is delivered. Tracking authorization status without manual follow-up consuming staff time.
These tasks share a common characteristic: they require interpreting payer requirements, not just retrieving or transmitting data. An EHR can surface a patient's coverage information. It cannot tell a coordinator whether a specific Blue Cross plan requires auth for this CPT code, what documentation criteria their reviewers apply, or whether those criteria changed last month.
That interpretation step — the translation of payer policy into actionable coverage intelligence — currently happens through a combination of staff expertise, portal research, phone calls, and institutional memory. It works inconsistently. It doesn't scale. And when it fails, the failure doesn't become visible until a denial lands weeks later.
Why this gap has persisted
The coverage workflow gap is not new. Specialty practices have been managing it manually for decades. The reason it has persisted isn't that no one noticed — it's that the problem resisted easy categorization.
It isn't clearly a clinical problem, so EHR vendors haven't owned it. It isn't clearly a transmission problem, so clearinghouses haven't owned it. It isn't clearly a billing problem, so RCM platforms haven't owned it. It sits in the seams between all three — which meant it fell to staff to absorb.
The operational consequence has been significant. A 2023 AMA survey found that prior authorization alone consumes an average of nearly two full business days of physician and staff time per week per practice. That burden doesn't reflect inefficient staff. It reflects a workflow with no technology layer responsible for making it intelligent.
A more complete model of the revenue cycle stack
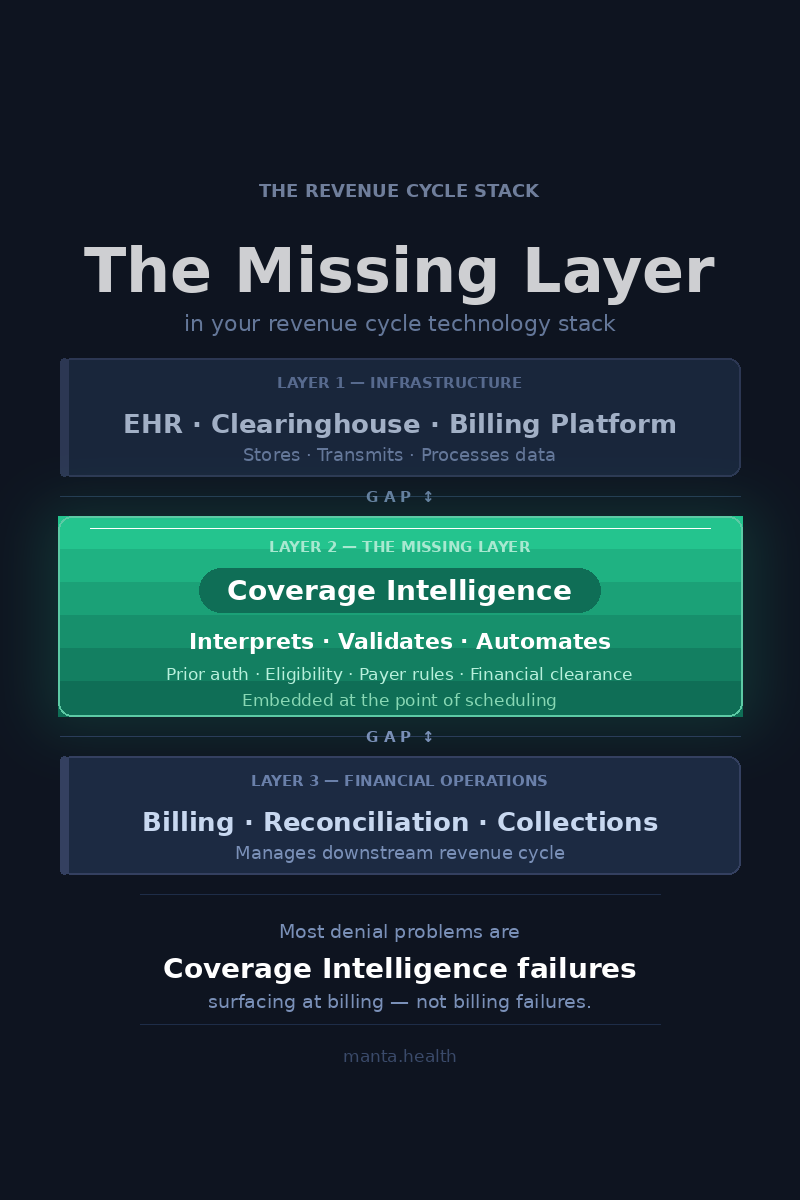
The revenue cycle technology stack is better understood as three distinct layers, not two:
- Infrastructure systems — EHRs, clearinghouses, and billing platforms. They store, transmit, and process clinical and financial data. These are the foundation and they are not going anywhere.
- Coverage Intelligence — the layer that interprets payer requirements, validates coverage conditions in real time, and automates pre-service authorization and financial clearance workflows. This is the missing layer. This is what Manta builds.
- Financial operations — billing, payment reconciliation, denial management, and collections. This layer becomes dramatically more effective when the coverage intelligence layer above it is functioning correctly, because fewer claims arrive broken.
The three-layer model matters because it changes how practices diagnose revenue problems. A high denial rate is not automatically a billing problem — it is often a coverage intelligence failure that surfaces at billing. A slow authorization cycle is not automatically a staffing problem — it is often an interpretation problem that no amount of headcount solves.
What changes when the gap is filled
When coverage intelligence is embedded in the pre-service workflow — not bolted on as a separate lookup step, but integrated at the point of scheduling — three things shift.
- Authorization requirements become visible before they become problems. A coordinator booking a procedure knows at scheduling whether auth is required, what documentation will be needed, and whether any flags exist on that payer-plan combination. There is no discovery phase. There is no last-minute assembly.
- Documentation is assembled against validated criteria. Because the system knows what the payer requires before the clinical team finalizes notes, documentation can be aligned to review criteria proactively rather than retrofitted after a pend or denial.
- First-pass approval rates improve structurally. Not because the process moved faster, but because submissions arrive complete. The delay was never in the payer's review queue — it was in the preparation gap that created incomplete submissions in the first place.
The diagnostic test for your own stack
If your practice has a coverage intelligence gap, these questions will be hard to answer with precision:
- What percentage of your prior authorizations are approved on first submission, broken down by payer and procedure?
- When a payer updates its authorization requirements for a procedure, how does your team find out — and how quickly does that change reach the staff submitting requests?
- How much time does your team spend each week on manual payer follow-up for authorization status?
If any of these are answered with "we track it loosely" or "we find out when we get denials" — the gap is active and it is costing you revenue that never appears in a denial report because it was written off, rescheduled, or simply never billed.
Practices that have closed this gap have seen measurable results — Rocky Mountain Eye Center reduced prior authorization approval time by 75% and cut their denial rate to 1.9%, while Northstar Medical Management reduced payer phone calls by 93% and cut PA determination time to under 10 seconds.
Final Thoughts
The category that fills the gap
Coverage Intelligence is not a feature of your EHR. It is not an add-on to your clearinghouse. It is a distinct layer of the revenue cycle stack with a distinct job: to ensure that every coverage decision made before a claim exists is made with complete, accurate, real-time information.
Manta Health builds this layer for specialty procedural practices — the organizations where authorization complexity is highest, payer rule variability is greatest, and the cost of a coverage intelligence failure is measured in rescheduled procedures and unbillable OR slots, not just administrative friction.
The stack most practices are running was built for a different era of revenue cycle complexity. Coverage Intelligence is what the modern stack requires.
See how the Coverage Intelligence layer works inside a specialty workflow - Book a Demo









-cropped.svg)
.svg)